.
Obstructive defecation, is a condition where despite straining the rectum is unable to empty its contents. This can be due to:
- Rectocele, where the rectum balloons outwards due to weakened walls;
- Enterocele, where loops of small bowel fall into the space between the vagina and rectum leading to bulging into these structures;
- Pelvic floor descent, where the weakened pelvic floor descends further than it should with straining;
- Rectal prolapse where the walls of the rectum collapse inwards (partial thickness) or collapse and fall out external to the anus (full thickness).
Frequently more than one condition occurs at the same time, and in rare cases all four conditions can be present.
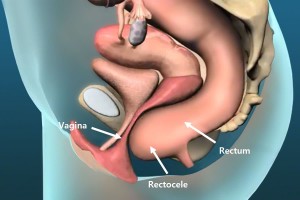
Rectocele
A rectocele results when the rectum bulges outwards on straining (figure 1). It is more common in women, and typically the bulge is at the front (anteriorly) into the vagina. It can result in the urge to apply pressure to the back (posterior) vaginal wall to facilitate evacuation.
Enterocele
Enterocele is where small bowel prolapses between the vagina and rectum causing bulging into and compression of the rectum (figure 2). It can also bulge into the vagina. If severe, the symptoms can be vomiting and abdominal distension due to small bowel obstruction.
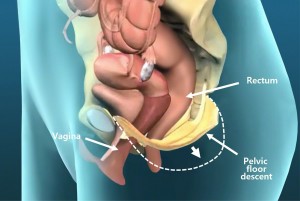
Pelvic floor descent
Pelvic floor descent is where on straining the weakened pelvic floor descends lower than it should (figure 3). This lack of fixation of the pelvis means that adequate intra-abdominal pressures cannot be obtained with straining sufficient to compress and empty the rectum.
Rectal prolapse
Rectal prolapse can be partial thickness and internal, where the lining (mucosa) of the rectum is mobile and falls into the lumen of the rectum obstructing flow, or can be full thickness and external with visible protrusion of rectum and mucosa through the anus. This often results in perianal moisture, bleeding, and some incontinence.
Symptoms
The main symptom of all of these conditions is a feeling of incomplete evacuation of the rectum on straining. Frequently, this leads to the feeling that one needs to evacuate again soon after the last attempt. This feeling can at times be so overwhelming, that a compulsion to digitally self-evacuate the rectum occurs. Full thickness rectal prolapse is often associated with perianal moisture, bleedings and incontinence.
Diagnosis
The diagnosis is often suspected based on clinical history and examination. Defecating proctography can be very useful for documenting and determining the exact cause and severity of obstructive defecation.
Ventral rectopexy
Ventral rectopexy is a procedure where a piece of bio-dissolvable mesh is used to anchor the pelvic floor and anterior wall of the rectum to the bony sacral promontory of the pelvic brim (see figure 3). This procedure is often required for patients with confirmed obstructive defecation due to partial or full thickness rectal prolapse, rectocele, enterocele and/or pelvic floor descent.
Robotic ventral rectopexy
Robotic ventral rectopexy (RVR) with the daVinci platform is gaining increasing popularity for the management of disorders that cause obstructive defecation, due to the increased ease with which suturing is able to be performed using the robot within the narrow confines of the bony pelvis. This is largely due to the ability of the articulating miniature robotic arms to perform complex fine-motor movements within a confined space.