Ingrown toenail is an abnormally curved toenail that grows into the adjacent skin causing pain, irritation, and inflammation.
Cause
Frequently there is a family history suggesting genetic factors. Shoe wear can also cause ingrown or painful nails.
Conservative Management versus Surgery
In the first instance ingrown toenail can be treated conservatively by cutting away the offending nail spicule avoiding tights shoes. Surgery (in the form of Wedge Resection) is required for persistent cases that fail to respond to conservative measures.
Wedge Resection
In persistent cases, where ongoing pain or infection is an issue, then surgery in the form of a Wedge Resection of the ingrown toenail, may be required. This involves:
- everting the ingrown nail,
- incision of the nail vertically,
- removal of the underlying germinal matrix, and
- curetting to ensure all matrix removed.

Surgery under Local Anaesthetic
The procedure can be performed under local anaesthetic or under general anaesthetic.
If your procedure is performed under local anaesthetic, you will receive a local anaesthetic digital block to number the entire toe that is being treated. The procedure is conducted in the clinic rooms under strict sterilisation to minimise the risk of infection. A tourniquet is applied to the toe to minimise bleeding during the surgery. The offending portion of ingrown toenail will then be everted, incised vertically, with the underlying germinal matrix also removed, with curetting performed to ensure all matrix attached to the proximal phalanx is also removed. A bandage and Elastoplaste dressing is applied, and the tourniquet released.
Surgery under General Anaesthetic
If your procedure is performed under general anaesthetic, the same conditions as above apply, except that your procedure will occur in a hospital and will be asleep during the procedure. You will not be able to drive a car or operate machinery until the following day after your surgery.
Mobility
You should be able to walk straight away following the surgery however it is advisable to have someone to assist you to get home.
Footware
It is recommended that you wear thongs or larger than normal shoes (e.g. Crocs) for the first week or two after your surgery. It is best to wear socks to avoid exposure of the toe to dirt and moisture.
Antibiotics
Typically, you will be given antibiotics for 5 days after your surgery. Usually Dicloxacillin or Flucloxacillin 500mg four times a day is recommended if there is no history of Penicillin Allergy.
Pain relief
Minimal pain relief medication is usually required however this can be discussed with your surgeon. Usually paracetamol (Panadol) and ibuprofen (Nurofen) are sufficient to control pain. Sometimes a strong pain killer such as tapentadol (Palexia IR 50mg) is required.
Dressings
Dressing are left in place and kept dry for one week. Your surgeon will remove your dressings and sutures one week after your surgery.
Washing
It is imperative that you keep you dressings dry in the first week after your surgery. During bathing or showering the entire involved foot should be placed in a water-proof bag with adhesive tape applied tightly to ensure water proofing. Be careful when showering that water does not enter the bag. You may stand “like a stalk” with the affected leg bent at the knee, to prevent shower water from entering the bag .
Chlorsig Ointment
Once the dressings are removed, daily application of Chlorsig (chloramphenicol) ointment is indicated for a further 1-2 weeks. It is recommended that the toe have a simple band aid applied daily to cover the wound, and that the affected toe remain covered with a sock to reduce risk of exposure to dirt or excessive perspiration moisture.
Risks and complications
There are a number of risks and complication following this surgery that, although exceedingly rare, you should be aware of and that you should discuss with your surgeon prior to undergoing wedge resection surgery. These are presented below:
Ischaemia
Prolonged application of the tourniquet can lead to distal toe ischemia. Patients with distal toe ischemia usually present with duskiness, poor healing, occasional ulceration, and even necrosis of the affected digit. Ingrown toenail removal can be performed without a tourniquet, but it is easier with a bloodless surgical field. If a tourniquet is used, it should be removed as soon as possible.
Dressings applied too tightly can also cause ischaemia to the tip of the affected toe. For this reason capillary return to the tip of the toe can be a reliable test to see if blood supply is adequate. If on pressing, the toe blanches (turns white) and refills with blood (turns red) within 3 seconds, this is adequate. If it takes longer than 3 seconds, the dressings may be too tight and should be loosened.
Bleeding
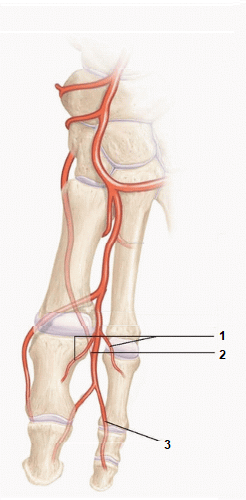
Distal branches of the dorsal metatarsal artery can be injured during wedge resection due to their close proximity to the germinal matrix attachment to the proximal phalanx. This may result in bleeding. For this reason the procedure is usually performed with a tourniquet.
Ischaemia (lack of blood supply) to the tip of the toe is uncommon, as there are usually sufficient other (collateral) arteries including the plantar digital arteries that supply the tip of the toe.
Bone destruction or infection
Overaggressive Electrocautery or Curetting to the Nail Matrix Can Damage the Underlying Tissues. Prolonged or high-current cautery has the potential to damage the fascia or periosteum underlying the nail matrix. If the toe is healing poorly several weeks after the procedure, your surgeon may consider debridement, antibiotics, and possible radiographic evaluation to exclude underlying osteomyelitis.
Infection in the first week or two after wedge resection can occur, and presents with a red, swollen, inflamed or hot toe. Infection is not unusual after the procedure, and oral antibiotics can be liberally administered. Some surgeons routinely prescribe antibiotics (e.g. Dicloxacillin or Flucloxacillin) for five days after the procedure. Management of aggressive infection can reduce the chance of patients developing the rare complication of osteomyelitis.
Regrowth of Spicule of Nail
The Patient Complains That the Surgery Did Not Get Rid of the Ingrown Nail. If inadequate matricectomy is performed, a spike of nail can regrow along the new lateral nail fold. This laterally growing piece of nail creates another inflammatory reaction in the lateral toe, necessitating a second procedure. The surgeon must make sure that the lateral horn matrix cells under the proximal nail fold are adequately ablated the first time.
Disfigurement
You may be surprised at the new look of your narrower toenail after wedge resection. In addition, the concavity left when the lateral granulation tissue is removed can be a shock, but patients can be reassured that the tissue will gradually fill in.
Call your surgeon if any of the following occur:
- severe pain not relieved with simple anaelgesics.
- poor capillary return to the tip of the operated toe
- red, hot or warm toe (may indicate infection)
- dusky, black appearing toe (may represent ischaemia)
- excessive bleeding (more than a teaspoon of blood)
- dressing gets wet
- dressings get smelly
- it has been more than a week since your surgery and the dressings have not been removed yet.